
Have you or someone you know had a stent placed in a coronary artery? After such a treatment, we often think that now the problem is completely solved, that the coronary artery will not become blocked again. However, sometimes, a small blockage or narrowing can occur again at the same place where the stent was placed, that is, in the same part of the artery that was treated. That is what doctors call 'In-Stent Restenosis'. Although the name may sound a bit complicated, it is actually quite simple. Let's talk about this in detail, in Sinhala that you can understand.
First, let's understand these words, shall we?
Before we talk about 'in-stent restenosis', let's understand the meaning of a few terms. Then it will be clearer to you.
What is 'Stenosis'?
Simply put, 'stenosis' is a narrowing or narrowing of a blood vessel in our body. Imagine that over time, dirt and rust build up inside a water pipe, blocking the flow of water.
So, what is coronary artery disease (CAD)?
Our heart also needs blood to function. We call the main arteries that supply blood to our heart the coronary arteries. CAD is when fatty deposits called plaque build up inside one or more of the coronary arteries, narrowing the arteries. This is also called atherosclerosis. Some people also call it "hardening of the arteries." This fatty buildup happens gradually, and may not show any symptoms at first. But if left untreated, it can lead to serious conditions like heart attack and heart failure.
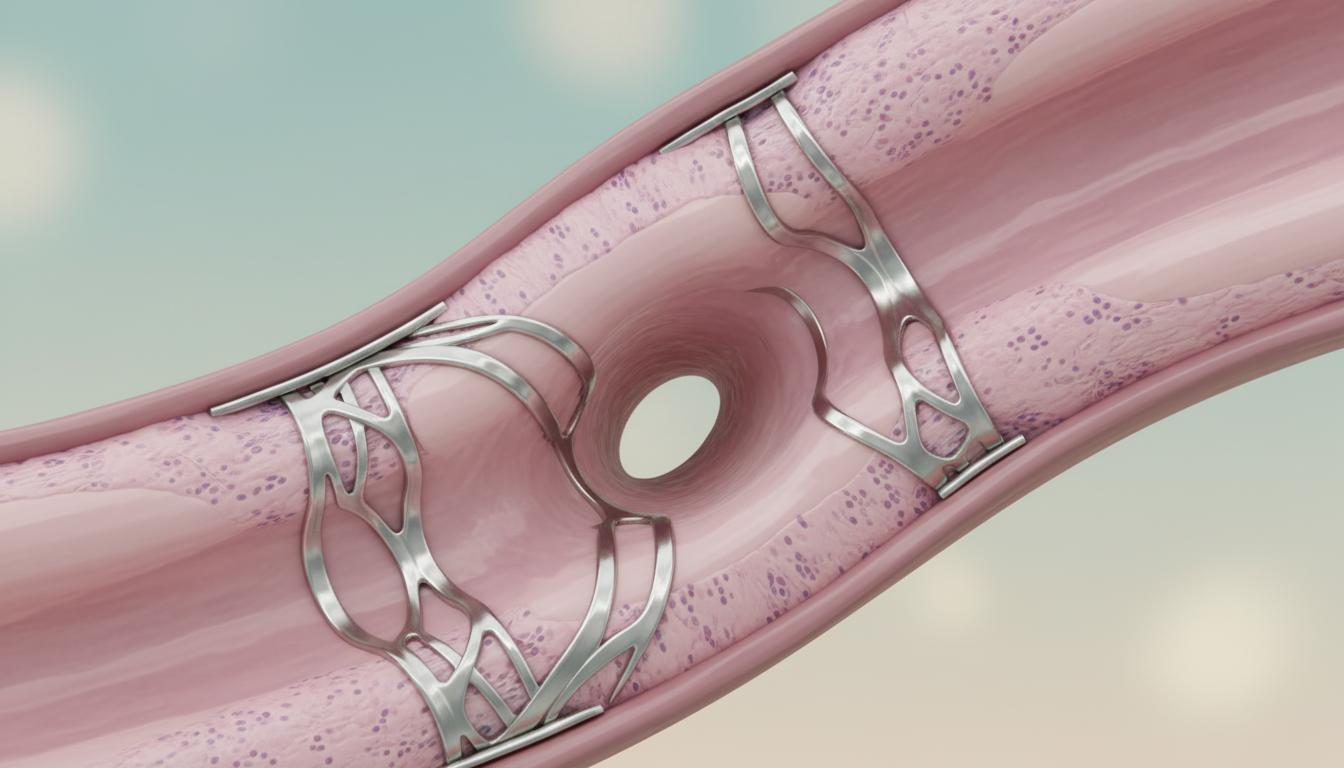
What are 'Angioplasty' and 'Stent'?
One of the main treatments that doctors use to open up blocked coronary arteries due to CAD is called angioplasty. Sometimes it is also called percutaneous coronary intervention (PCI). In this, a thin tube (catheter) is inserted through a small hole in the skin into the blocked artery. A small balloon-like device at the end of the tube is inflated, widening the blocked artery. Then, to keep the artery from collapsing again and to keep blood flowing properly, a small mesh tube – that's what a stent is for – is placed inside the widened artery. Then, blood flows smoothly again.
Okay, now what is this 'In-Stent Restenosis'?
Now you understand why and how a stent is placed. After a stent is placed and the blood flow is restored in the coronary artery, sometimes the artery starts to narrow again right where the stent was placed, that is, inside the stent. That's why we call it 'In-Stent Restenosis'. 'Re' means "again", and 'stenosis' means "narrowing". So, this means "narrowing again inside the stent".
How common is this condition?
Now you might be wondering if this is something that happens to everyone who has a stent. No, it doesn't happen to everyone who has a stent. But, roughly speaking, about 1 in 4 people who have a stent have some chance of developing this condition called `In-Stent Restenosis`. It usually happens within three to six months of having the stent placed.
Important: If you have balloon angioplasty without stenting, the risk of restenosis is even higher. About 4 in 10 people will have their artery blocked again.
Why does 'in-stent restenosis' occur?
It's a really interesting question. After a stent is placed, our body tries to "heal" it. That is, a new layer of cells (a ``new lining``) grows over the stent, making the inside of the vein smooth again. This is actually a good thing, because then the blood can flow more easily without clotting.
However, sometimes, under this new layer of cells, around the stent, a little too much scar tissue grows. When this scar tissue grows too much, the inner lining of the artery thickens, narrowing the blood flow again. This is the main cause of `In-Stent Restenosis`.
Remember, this usually happens within three to six months of stenting. After that, the risk of scar tissue forming and blocking the vein is very low.
Who is at higher risk of developing 'in-stent restenosis'?
Although anyone who has a stent placed for CAD can develop this condition called `In-Stent Restenosis`, some people are at a slightly higher risk. Let's take a look at who they are:
- For people with high blood cholesterol levels. (This is what contributes to many heart diseases!)
- For those with kidney disease .
- For those who smoke. (This is definitely something you should stop doing!)
- For those with poorly controlled diabetes .
- For those with uncontrolled high blood pressure (hypertension).
If you have these conditions, it is very important to talk to your doctor and get them under control.
What are the symptoms of 'in-stent restenosis'?
Most of the time, people with `In-Stent Restenosis` do not show any outward symptoms. That is why it is very important to see your doctor at regular intervals and undergo the necessary tests after having a stent placed.
However, some people may develop symptoms. If they do, the symptoms are often similar to those of pre-existing CAD. These include:
- A feeling of pain, tightness, or discomfort in the chest. We call this ``angina.'' This chest pain may get worse when you exercise, climb stairs, or become slightly tired.
- Cold sweat.
- Dizziness, lightheadedness, or feeling faint.
- Excessive fatigue and weakness.
- Feeling an abnormal heart rate (`Heart palpitations`).
- Nausea.
- Shortness of breath, sometimes even when walking a short distance.
- Pain in the shoulder or arm (especially the left arm).
If you have these symptoms, you should see a doctor without wasting time.
How is 'in-stent restenosis' diagnosed?
As I have said before, since `In-Stent Restenosis` does not always show symptoms, it is essential to see your doctor regularly after a stent is placed. Then, the necessary tests can be done.
If you have symptoms, your doctor may recommend tests like these:
- Exercise stress test : This test measures how your heart pumps blood and looks for changes in your ECG as you walk on a treadmill or ride a bike.
- Cardiac catheterization and angiogram : This is done before the stent is placed. This can be done again to see exactly if there is a blockage inside the stent.
- Coronary computed tomography angiogram (CCTA): This is similar to a CT scan. A special dye is injected into the heart to create 3D images of the heart's arteries.
- Fractional flow reserve (FFR): This can be done at the same time as the angiogram. A special wire is inserted into the vein and the blood pressure is measured on both sides of the blockage to see how severe the blockage is.
- Intravascular ultrasound (IVUS): This can also be done at the same time as an angiogram. A small ultrasound probe is passed into the vein, allowing the inside of the vein wall and stent to be seen very clearly.
What are the treatments for 'in-stent restenosis'?
Your doctor will determine the most appropriate treatment for you based on the severity of your In-Stent Restenosis, that is, how narrowed the artery is, and your overall health. It may include one of the following treatments:
- Medications: To control symptoms such as angina caused by In-Stent Restenosis, the dosage of current medications may be increased or new medications may be added.
- Repeat angioplasty: The blocked artery is widened again with a balloon, and sometimes another stent is inserted. Sometimes a drug-coated balloon may be used.
- Heart bypass surgery: This is also called coronary artery bypass grafting, or CABG. This is a major operation. It involves creating a new path for blood to flow around a blocked artery. This means that a piece of artery from another part of your body (such as your leg or chest) is taken and connected to the blocked artery.
- Vascular brachytherapy: This is a slightly different treatment. Similar to radiation therapy used to kill cancer cells, this involves giving a small amount of radiation for a short period of time to the stent to stop the scar tissue from growing back. This is also called coronary brachytherapy.
Are there ways to prevent 'in-stent restenosis'?
Yes, the good news is that the risk of `In-Stent Restenosis` can be reduced. One of the main ways to do this is by using drug-eluting stents (`DES`).
These `DES` are different from bare metal stents (BMS). They have a thin coating of medicine on them. Once the stent is inserted into the vein, the medicine is gradually released, controlling the formation of scar tissue and the growth of cells.
Years ago, there was talk about the risk of blood clots with these `DES`. However, the new generation of drug-eluting stents is very safe and very effective. When using these `DES`, the risk of `In-Stent Restenosis` is significantly reduced. Roughly speaking, `Fewer than 1 in 10 people` develop `In-Stent Restenosis`.
Therefore, if you are going to have a stent placed, talk to your doctor to decide what type of stent is best for you.
What is the outlook for someone with 'in-stent restenosis'?
If you develop `In-Stent Restenosis`, you may be slightly more likely to experience potentially life-threatening heart conditions, such as `unstable angina`, `acute coronary syndrome`, and `heart attacks`.
Fortunately, these risks have been greatly reduced with the advent of new stents (especially DES) and improved stent placement techniques. In addition, there are now effective treatments for In-Stent Restenosis.
If you have CAD, you should follow your doctor's instructions exactly to prevent In-Stent Restenosis and protect your heart in general. That means:
- Reduce your salt intake and take the medications prescribed by your doctor (especially those for blood pressure, cholesterol, and blood clotting) exactly and on time.
- Limit your alcohol consumption. If you are addicted to alcohol, seek help to overcome it.
- Eat a heart-healthy diet . Eat less oil, sugar, and flour, and more vegetables, fruits, and fiber-rich foods.
- Be aware of the types of fats you eat. Reduce your intake of foods high in saturated and trans fats (fast food, fried foods, packaged foods) as much as possible.
- Maintain a healthy weight. Exercise daily.
- If you have diabetes, control it well.
- If you smoke, try to quit today. There are ways to get help.
When should I call a doctor?
If you think you are having a heart attack (symptoms such as severe chest pain, shortness of breath, sweating), call the 1990 Suwaseriya Ambulance Service immediately.
If you have had a stent placed before and these symptoms recur, see your cardiologist immediately:
- Chest pain (angina), tightness, pressure, pain in the arm or shoulder.
- Cold sweat.
- Difficulty breathing, wheezing.
- Excessive tiredness or weakness for no reason.
What should I ask my doctor?
When you meet the doctor, you can ask questions like these to get a clear understanding of your condition:
- Why did I get this `restenosis`? What are my risk factors?
- Can I get restenosis again? What should I do to prevent it?
- What lifestyle should I follow to protect my heart?
- What signs of complications should I look out for?
- What is the best treatment for me?
Finally, what to remember (Take-Home Message)
Okay, so the most important thing you need to remember from what we've talked about is this. Angioplasty and stenting are two of the most important and life-saving treatments for heart disease. These treatments improve blood flow to your heart, reduce the symptoms of CAD, and improve your quality of life.
However, if symptoms such as fatigue, chest pain, and shortness of breath reappear after a stent is placed, it could be a sign of `In-Stent Restenosis.` If that happens, don't panic or delay, but definitely see your doctor for advice.
Fortunately, the new, safer drug-eluting stents available today have greatly reduced the risk of developing In-Stent Restenosis. There are also good treatments for this. It is best to talk to your doctor about what type of stent and treatment is right for you. Take care of your heart!
` Stents, in-stent restenosis, heart disease, angioplasty, coronary artery disease, coronary artery disease, heart attack
💬 අදහස් (0)
තවමත් කිසිදු අදහසක් පළ කර නොමැත. ඔබේ අදහස පළමු වරට මෙහි එක් කරන්න.
ඔබේ අදහස එක් කරන්න